
Scientists Think They Know Why Some People Can’t Poop – And It Starts in The Gut’s ‘Second Brain : ScienceAlert
Enjoying consistent, low-effort bowel movements is a massively underappreciated aspect of one’s quality of life.
Yet this is not the case for up to 15 percent of the global populace, as millions of individuals struggle with chronic constipation.
The constipation umbrella – thankfully a figurative term – comprises different subtypes with various causes and symptoms.
This includes slow-transit constipation (STC), the reduced motility of last night’s (or week’s) steak through the gastrointestinal tract, potentially caused by abnormalities in the enteric nerves that control peristalsis, the rhythmic muscular contractions that push the poop-to-be from throat to anus.
As detailed in a recent study published in Frontiers in Immunology, constipation cases like STC may manifest from a misbalance in the gut-brain axis that controls daily factors like mood and possibly even cognitive decline.
Yet this enigmatic imbalance is affected by ever-shifting interactions between the gut microbiota, the mucus membranes of the gastrointestinal tract, and the enteric nervous system (ENS), also known as our body’s ‘second brain.’
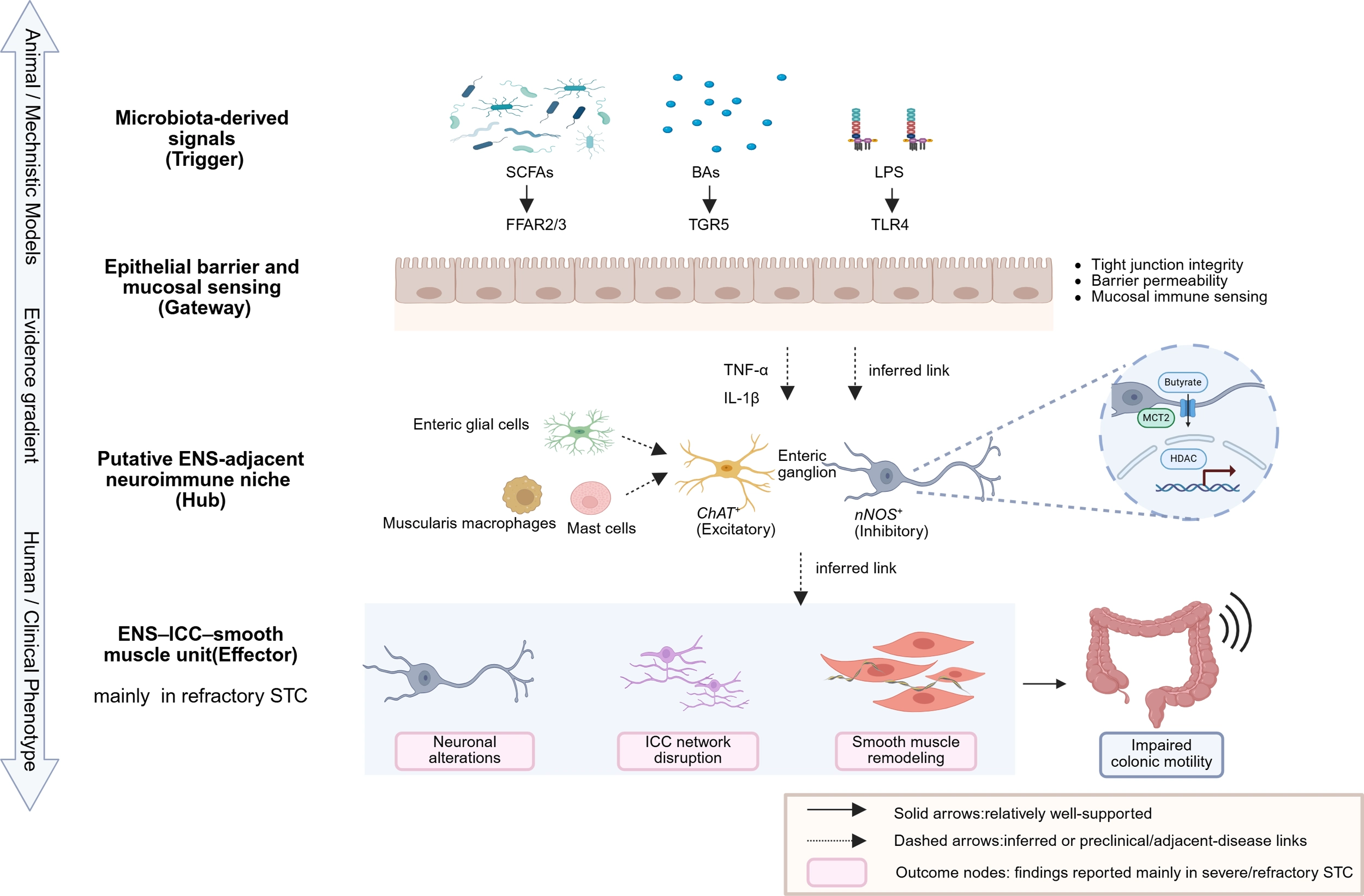
To organize this interplay, the researchers propose a tongue-twisting “Trigger–Gateway–Hub–Effector framework” which integrates fragmented evidence from human, animal, and in vitro data.
In this framework, the “Trigger” is gut dysbiosis. As the microbial populations change, possibly due to diet, medications, or other lifestyle factors, they produce different metabolites, or microbial byproducts.
These metabolites act as molecular signals, potentially affecting the intestinal epithelial barriers, the bouncers of the gut, which selectively allow nutrient absorption while keeping toxic compounds out of the bloodstream.
“Current evidence supports an association between gut microbiota changes and [constipation],” the researchers say.
“But the overall evidence remains moderate. It mainly comes from human observational studies and experimental models, not direct human mechanistic data.”
Yet some microbial compounds appear clearly beneficial, including the gut-boosting short-chain fatty acids generated as microbes ferment dietary fiber.
Prominent metabolites may also include those derived from the fat-emulsifying bile acids produced in the liver; inflammatory lipopolysaccharides from bacterial membranes; and byproducts of the turkey-famous tryptophan, which turns into the ‘feel-good’ chemical serotonin.
Altered metabolism of such compounds may not directly cause constipation, but may create a “permissive environment” that weakens membranes and immune mechanisms, such as gut mucus.
These membranes of the intestinal epithelium are the “Gateway” in the researchers’ model.
A leaky gut may then allow microbial metabolites to trigger inflammation and disrupt immune and neuromuscular functions in the gut, as in disorders like irritable bowel syndrome (IBS).
“Clinically, barrier vulnerability is therefore best interpreted as a permissive condition that may enable or amplify downstream immune–ENS interactions rather than as an independent driver of motility failure,” the researchers note.

Next, the “Hub” represents the microenvironment around the ENS, where signals from neurons, support cells, connective cells, immune cells, and microbes are locally integrated.
The resultant chaos of these bidirectional communications can harm the muscularis externa, the poop-propelling layer of intestinal smooth muscle that helps control motility via peristalsis.
The endpoint in the researchers’ model is described as the “Effector,” or the ENS itself, “through which microbiota-associated, epithelial, immune, and glial signals may converge to influence gastrointestinal motility.”
This may lead to neuronal loss, neurochemical imbalances, or disruptions of the ‘pacemaker’ cells that generate electrical waves driving the stool-squeezing gut rhythms of peristalsis.
Due to this complicated cascade, and the heterogeneity of constipation cases, multiple therapeutic avenues warrant further exploration.

Treatments may focus on correcting dysbiosis through supplementation with microorganism-loaded probiotics and the prebiotics necessary to feed them – though such remedial options don’t always need to enter through the mouth, as fecal transplants have shown promise in treating various disorders.
Other strategies, informed by research on disorders like IBS, could target immune function to reduce inflammatory signaling.
Similarly, protecting neurons or ‘pacemaker’ cells in the ENS microenvironment could improve motility, though no such therapies have yet been established for constipation.
Related: How Long Poop Stays in Your Body May Impact Your Health, Study Finds
Furthermore, these healthcare techniques may be used in conjunction, rather than as standalone therapies, potentially alongside traditional laxatives that improve motility and stool hydration.
“From a translational standpoint, this integrative perspective supports an evidence-weighted therapeutic paradigm encompassing modulation of the gut microbiota, regulation of immune or glial responses, and preservation of neuromuscular function,” the researchers conclude.
This research was published in Frontiers in Immunology.
This article was fact-checked by Michael Irving and edited by Rebecca Dyer. While we pride ourselves on our process, we are only human. If you spot a mistake, please let us know.
