
This week Tony Wyss-Coray and I published an invited review paper in Nature Medicine entitled “Biological Aging Clocks in Health and Disease.” The concepts and content of the paper may be difficult to understand for people not working in life science, but they are groundbreaking and have exciting implications for the future of medicine. So this edition of Ground Truths is intended to make all of the progress comprehensible for you and to hopefully see the coming inflection point in medicine. I’ll divide this into 4 key sections: (1) the chronological illusion of aging; (2) aging is synchronous in our body—the value of organ clocks, (3) cell clocks and the master regulators of aging; and (4) impact for routine medical practice.
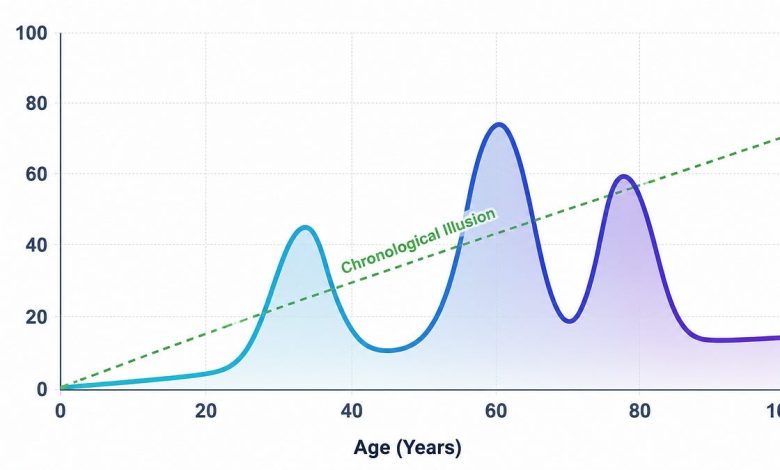
It is well recognized that each of us age at a different pace, exemplified by person aged 90 who has never been sick and physically appears to be decades younger (what we’ve called the Wellderly or Super Agers). But the overall assumption has been that all of us undergo a gradual, steady, linear process of aging, predictable wear and tear throughout lifespan, as assessed via the calendar. That “chronological illusion” (the dotted line below) has now been debunked. Multiple studies that used large-scale proteomics (proteins or other omics/biological metrics and imaging) and have found 3 major waves of aging that occur around ages 34, 60 and 78 years, as shown below.

It also turns out our organs age at a different pace. We might not have known that without the ability to do high-throughput proteomics with AI analytics. By that I mean being able to assess up to 11,000 proteins from a tube of blood and use AI to define which proteins are tracking which organ and the immune system. Perhaps the best way to prove this asynchronous process within our body is from the world’s oldest longitudinally followed birth cohort— the UK’s National Survey of Health and Development (NSHD). All of the 1,800 participants were born in the same week in 1946. At age 63, proteomics were assessed for 6 organs and the immune system. In the Figure below, you can see there is about a 10-year spread of organ and immune system pace of aging among the cohort. Conventional, top left, refers to whole body, that is all measurable age-related proteins without breakdown by organ.

Within participants there were differences in the chronological age compared the person’s organ age. In the example below, the heart shows accelerating aging. Multiple studies of organ clocks have correlated fast aging of an organ with a disease indexed to that organ, such as heart to heart failure or brain to Alzheimer’s disease.

This pattern of asynchronous organ-specific aging has been noted in several proteomic studies, and has been shown to correlate with lifestyle factors (such as alcohol intake and liver age) and as I previously reviewed in Ground Truths hormone replacement therapy and the immune system age. To give you a sense of the breadth of what organ clocks tracked in the NSHD cohort, from the paper: “The organ clocks were adversely affected by overweight in adolescence, lack of education, smoking and various types of adversity across the life course (such as parental divorce or lack of social support). In contrast, there were several healthspan-protective factors including normal birthweight, higher childhood socioeconomic status, sustained physical activity and moderate alcohol intake.”
Discovering organ clocks can be considered a breakthrough in their own right. But it goes deeper—to cell clocks. Frankly, I would not have expected we could track aging for different cell types, like brain astrocytes or microglia, from the proteins appearing in the blood. But that is what is now possible. This work was published just 2 weeks before our review and included in it. Over 40 cell types were assessed in over 60,000 individuals with over 7,000 proteins biological aging. About 1 in 4 participants had accelerated aging in 1 cell type. A compelling pattern was seen for many conditions, as illustrated below for brain astrocytes and the risk of Alzheimer’s disease (AD). People with accelerated aging (“old”) of these cells had a 12.6 fold higher rate of developing AD compared with slow (“young”) aging of astrocytes.

In a similar way to assess risk of young or old astrocytes, but now broken down by the known APOE4 risk allele, with 1 copy in the middle graph and 2 copies at the far right. You can see the minimal risk in the people without E4 (at left below, 2 copies of E3), risk of AD increased with old astrocytes in those with 1 E4 allele copy, but dramatically increased risk (nearly 40-fold) for old astrocytes vs young in people with 2 copies of the E4 allele. Noteworthy, the age of astrocytes predicted risk of Alzheimer’s independent of APOE4 status. It adds to p-tau217 and other neuroinflammation markers (p-tau181, NfL, GFAP) as a way to more precisely determine risk of Alzheimer’s disease. Put another way, simple people with APOE 4 are not at high risk for Alzheimer’s, but we didn’t have a way to know that before.

A consistent patten between organ and cell clock studies is that the more evidence for accelerated aging, reflected by more organs or cells, the more increased mortality during follow-up (or reduced survival), seen side-by side below for 2 cohorts (one showing mortality and the other survival).

The same pattern for aged cell types in the UK Biobank and relationship to survival is seen in the Figure below

The other key consistency is the prominence of the relationship of survival seen with 2 organ and cell types: the brain (neurons) and immune system (immune cells). When these exhibit normal paced aging, survival over 15-17 years approaches 100%. Accordingly, the brain and immune system have the appearance of master regulators of the aging process. They seem to be acting as systemic gatekeepers, supporting resilience despite extreme aging of other organs or cells. I’ve previously emphasized the interdependence of the brain and immune system. The brain can be viewed as “mission control” for the immune system.
It isn’t as if these organs and cell types are the only ones that are informative. That couldn’t be further from what has been seen. The aging of lung cells, smoking status, and the incidence of lung cancer, as shown below, is just another of many examples.

We’re not there yet to implement organ and cell clocks, but not far away. I’ve had my organ clocks assessed by one of the companies in beta phase testing. Beyond more than 10 studies cited in the review, much more validation of organ and cell aging clocks is currently underway. This month we are launching a randomized controlled trial in participants with high-risk of Alzheimer’s disease testing aggressive lifestyle improvement with 24/7 coaching to prevent the disease. All individuals will have p-tau217 and brain clocks assessed at baseline and follow-up. The main endpoint is reduction in p-tau217 after one year, which has been shown to be particularly mutable in small intervention studies with exercise (previously reviewed in Ground Truths). All of the data thus far suggest that organ clocks are eminently mutable too, influenced by lifestyle factors, medications, and many other perturbations as reviewed above.
Let’s take a step back on how this field of aging has evolved. The concept of metrics to assess biological aging got its roots more than 15 years ago with the seminal work by Steve Horvath and others assessing DNA methylation (epigenetic) clocks. Here’s my conversation about epigenetic clocks with Steve Horvath. That first generation was built on with other information, be it from plasma proteins or clinical data, to yield more refined molecular clocks. But only in the past few years, have we seen the field move from assesing human aging more holistically to getting specificity at the organ and cell levels. The Table below from our review summarizes what can be considered 6 generations of biological clocks.

This progress has implications for the practice of medicine and the potential for achieving reversal of aging. Detecting accelerated aging of an organ could enable a new path to prevention. Take a person with risk factors for heart disease who exhibits accelerated aging of his artery clock and/or blood vessel cell clock; there’s potential for a new dimension of risk to be ascertained. There is no shortage of means to help prevent atherosclerotic heart disease for such individuals. Perhaps more striking is a new window into the aging of our immune system, for which we have no way to assess in the clinic today, but now could be quantified at both the immune system and immune cell levels. That could provide the advance warning for the need to amp up the immune response, be it by lifestyle factors, vaccines or medications. And don’t forget that the same clocks can be used to assess the impact of the preventive strategy or intervention. For the 2-stage prevention of neurodegenerative diseases, the data from clocks would be added to other layers of data to assess concordance and directionality (Figure below, abbreviations PRS-polygenic risk score, EHR-electronic health record, MCI-mild cognitive impairment).

I won’t go through all the organs (or 40 cell types) but I hope this gives you the sense of enabling precision prevention.
There is considerable investment and excitement about partial cellular reprogramming (also known as “rejuvenation”) and other biotech interventions to slow the human aging process. Last month cellular reprogramming (with 3 of the 4 Yamanaka transcription factors) was initiated in a pilot trial of patients with advanced eye diseases. While that may show aging of retinal cells is slowed, it still would not demonstrate our ability to slow or reverse human aging. But comprehensive organ and cell clock assessment may ultimately provide surrogate endpoints to support efficacy and pre-empt many years of clinical trial follow-up. That’s much further away than using clocks in the clinic, but a realistic possibility if validation for such an approach is achieved.
We have a problem right now with some aging clocks. They (mostly methylation, epigenetic) are being sold commercially direct-to-consumer without standardization or reliability, and at considerable expense. I would suggest not buying any of these tests. The tests with the most potential are at the organ and cellular level, and none are commercial at this point. That will change in the next year, but will still require attention to adequate validation and standardization, and the need to bring the cost way down, which is possible when done at scale. We’ve seen that at the UK Biobank, which was able to do 6,000 plasma proteins (O-link)for approximately 500,000 participants at ~$50 a pop (original charge for O-link and Somascan was >$900 for each individual).
Like so many other biomedical advances I have recently reviewed, we’re seeing the product of very large datasets and AI analytics. That was the case for the 14-protein blood test predicting and preventing lung cancer, the breakthrough blood test for assessing the tumor microenvironment, and use of imaging the thymus for immune system health Add organ and cell clocks to that quickly growing list.
I hope I haven’t lost you along the way, as this post was fully intended to be practical, a translation of our publication with high density information and the usual jargon that makes it hard to ingest, especially for folks not grounded in this stuff. For those who have been following Ground Truths for the past few years, you will recall how excited I was about the discovery of organ clocks back in late 2023. The field has gone forward at torrent pace since then, with the added dimension of cellular clocks.

The transition from calendar to clocks in medicine will take longer than it should. It requires a structural shift in how we define age. It doesn’t mean we abandon
chronological age, but counting candles is fixed and will be transcended. Biological age is now measurable at a granular level and increasingly shown to be modifiable. I believe this represents the most important advance we have yet seen in the science of human aging. It paves the way for a great inflection for promoting health and preventing diseases in the future.
******************************
A big thanks to Ground Truths subscribers from every US state and 212 countries. Your subscription to these free essays and podcasts makes my work in putting them together worthwhile. If you’re not a subscriber, please join!
If you found this interesting PLEASE share it!
Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don’t hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.
Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. It enabled us to accept and support a record number of 51 summer interns here with us now! These are high school, college and medical students selected from thousands of applicants. We couldn’t do this expanded program without the funds coming in through Ground Truths.



